- A whole person care program integrates physical health, behavioral health, and social services into one coordinated model, rather than treating each as a separate system.
- Fragmented care creates costly gaps: when providers do not share information, patients receive duplicative, inconsistent, or delayed treatment.
- California's Whole Person Care pilot (2016-2021) demonstrated measurable results for high-risk Medicaid populations, including reduced hospitalizations and ER visits, and laid the foundation for CalAIM's statewide Enhanced Care Management program.
- For employers and health plans, whole person care directly addresses the conditions driving the highest costs: complex chronic conditions, untreated behavioral health needs, and high ER and specialist utilization.
- Effective programs require unified medical records, multidisciplinary clinical teams, and care delivery across multiple settings to close the gaps that fragmented systems routinely leave open.
A whole person care program coordinates physical health, mental health, and social needs together within a single, integrated care model, unifying what fragmented systems have historically treated as separate concerns. When these dimensions are managed in isolation, care gaps are inevitable: chronic conditions go unmanaged, behavioral health needs surface late, and social factors that directly influence clinical outcomes are overlooked entirely.
For employers and health plans managing populations with complex, high-cost needs, that fragmentation translates directly into higher utilization, avoidable acute events, and rising total cost of care.
This integrated approach addresses those dynamics at the structural level, offering a measurable path to better health outcomes and sustainable cost reduction across both commercial and Medicaid populations.
What Is a Whole Person Care Program?
A whole person care program integrates physical health, behavioral health, and social services under one coordinated framework. Rather than sending patients to separate providers operating in isolation, this model brings care together so that every clinician involved has the same information and works toward the same goals.
The problem this solves is well-documented. When a primary care physician has no visibility into what a specialist prescribed, or when a behavioral health provider is unaware of a patient's chronic condition, treatment decisions are made on incomplete information.
Those gaps produce worse outcomes and higher costs. A whole person health model closes them by treating the full picture of a person's health, including the social and behavioral factors that significantly influence clinical outcomes.
The Policy Foundation: California's WPC Pilot and CalAIM
This model gained significant traction through California's Whole Person Care (WPC) pilot program, launched by the Department of Health Care Services (DHCS) in 2016. The program coordinated physical health, behavioral health, and social services for high-risk Medi-Cal beneficiaries across 25 counties, serving nearly 250,000 enrollees through 2021.
The final evaluation, conducted by the UCLA Center for Health Policy Research, found that WPC enrollees experienced meaningfully lower acute care utilization compared to similar patients outside the program, including 45 fewer hospitalizations and 130 fewer emergency department visits (per cohort annually) per 1,000 beneficiaries per year.
DHCS built on these findings with CalAIM, which expanded and enhanced care management statewide and established coordinated care for complex populations as a standard expectation for Medi-Cal managed care plans.
For health plans operating under CalAIM, whole person care is not a differentiator; it is a compliance requirement. The infrastructure to deliver it effectively is what separates high-performing plans from those that struggle to meet Enhanced Care Management standards.
Why Fragmentation Is the Core Problem
Fragmented care does not just frustrate patients. It produces measurable financial and clinical harm. Providers working without shared records order duplicative tests, miss relevant history, and refer patients to specialists for problems that coordinated primary care could manage.
Behavioral health needs go unaddressed because no one is responsible for identifying them during a physical health visit. Social factors (housing instability, food insecurity, limited transportation) are left entirely out of the clinical picture, even though research consistently demonstrates their impact on health outcomes.
A whole person care program assigns accountability for all of these dimensions to one integrated team.
Why Employers and Health Plans Are Adopting Whole Person Care
Employers managing large, diverse workforces face a structural challenge: traditional benefits packages treat medical, behavioral health, and specialty care as separate products. Employees navigate these systems independently, often without guidance or coordination. The result is delayed care, avoidable ER visits, and untreated chronic and behavioral conditions that compound over time.
For managed care organizations serving Medicaid or Medicare populations, the challenge is similar in structure but more acute in scale. Members with complex needs, including those managing multiple chronic conditions, behavioral health disorders, or significant social risk factors, generate disproportionate costs.
Without coordinated care, they cycle through emergency departments and inpatient settings rather than receiving the proactive, longitudinal management that would keep them stable.
A virtual-first whole person care model addresses these dynamics directly. Multidisciplinary clinical teams, supported by clinical intelligence and comprehensive medical records, can manage the full spectrum of a patient's needs through one integrated platform: urgent concerns, chronic condition management, behavioral health, and coordination with social services where relevant.
The Financial Case
The financial impact of whole person care is well-established. Galileo has demonstrated an 11.5% reduction in total cost of care within six months of working with employers, driven by lower downstream utilization and stronger member engagement. Galileo members are over 70% less likely to require specialist appointments or ER visits.
These outcomes follow directly from the model's structure. When employees have reliable access to a clinical team that knows their history and coordinates their care, low-acuity concerns are resolved before they escalate.
Chronic conditions are managed proactively. Behavioral health needs are identified and addressed as part of routine care, rather than surfacing later as costly acute episodes.
Key Components of an Effective Whole Person Care Program
Not every program that claims to deliver whole person care does so in practice. The structural requirements are specific, and programs that lack any one of them tend to reproduce the fragmentation they are designed to solve. The following components are operationally necessary for the model to produce meaningful clinical and financial outcomes.
Unified Medical Records
Care quality depends on information quality. When a clinician has access to a patient's complete history, including previous diagnoses, medications, specialist notes, lab results, and behavioral health treatment, they can make faster and more accurate decisions. Without this, fragmentation persists even when the intent is coordination. Effective programs aggregate data from across care settings and make it available to every member of the clinical team in real time.
Multidisciplinary Clinical Teams
Whole person care requires more than primary care physicians. Effective teams include clinicians with expertise across behavioral health, chronic disease management, and complex care, supported by health advocates and care coordinators who manage transitions, follow-ups, and social service referrals. Galileo's team-based model operates across 20-plus specialties, with peer-reviewed case management ensuring consistent clinical quality across the population.
Care Delivered Across Multiple Settings
Populations with complex needs cannot always access care in traditional clinic settings. An effective whole person care program delivers across multiple modalities:
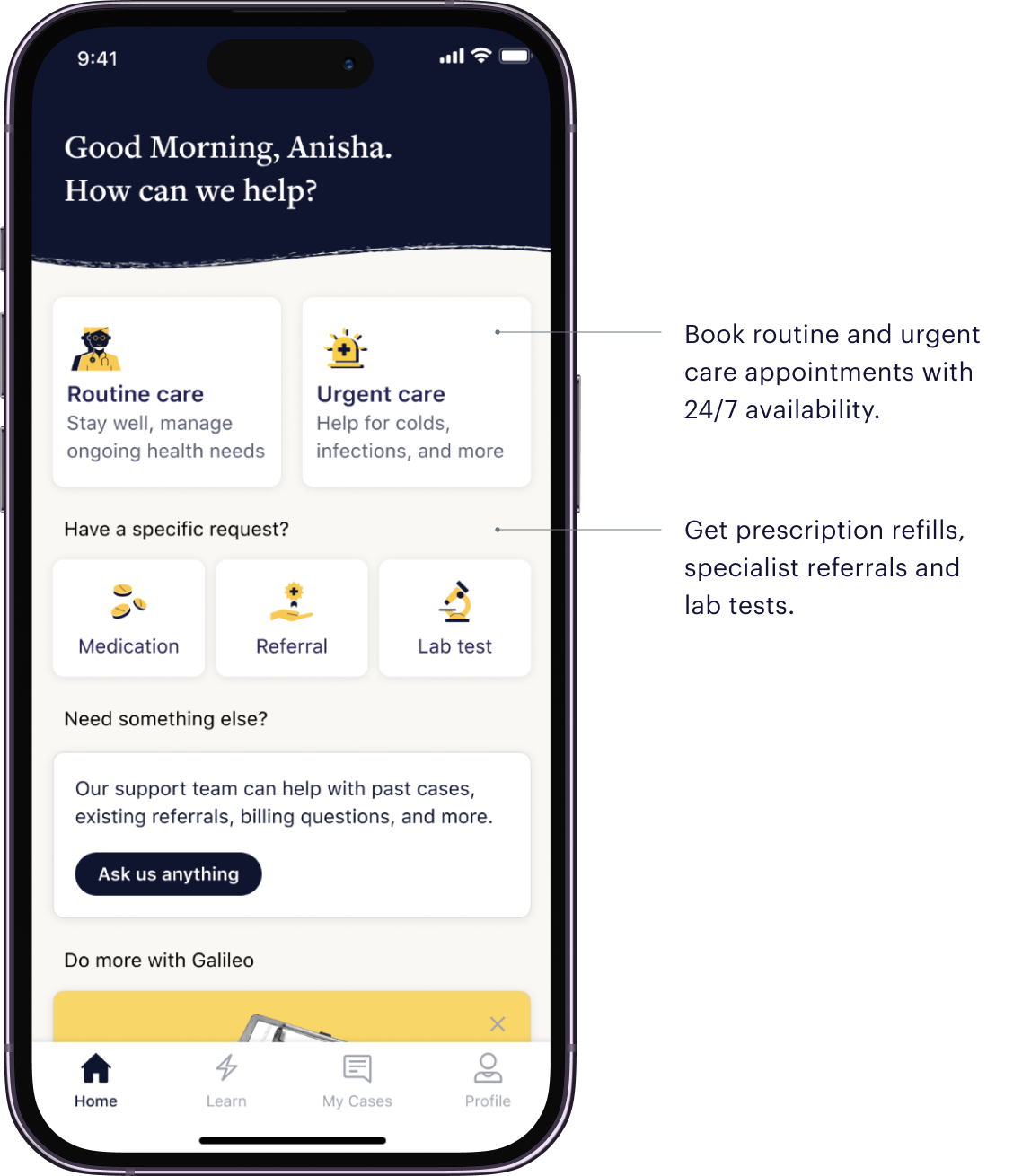
- Virtual (text, video, and phone): 24/7 access to clinical teams for the majority of care needs, without requiring patients to travel or take time off work.
- In the home: Specialized teams managing complex and chronic conditions for higher-acuity patients who benefit from direct clinical assessment.
- Mobile clinics: Community-based access reaching populations facing geographic, transportation, or mobility barriers.
- Care centers: In-person visits for cases requiring hands-on evaluation.
This multi-setting architecture ensures that care remains consistent and accessible regardless of a patient's circumstances, a prerequisite for serving the high-risk, high-need populations that whole person care programs are designed to reach.
Behavioral Health Integration
Behavioral health is not an add-on in an effective whole person care model. It is embedded in the primary care relationship. Galileo's clinicians are trained to identify and manage low-to-moderate acuity behavioral health needs, including anxiety, depression, and stress-related conditions, as part of routine care. Early identification and integrated behavioral health support reduce the likelihood that untreated behavioral conditions escalate into costly acute episodes.
Measuring Success in Whole Person Care
Effective whole person care programs are measurable. Defining the right metrics at the outset is essential to evaluating whether a program is delivering on its clinical and financial objectives.
Clinical Outcomes
For populations with chronic conditions, relevant metrics include control rates for conditions such as diabetes (HbA1c) and hypertension (blood pressure), medication adherence, rates of preventive screening completion, and follow-up visit compliance after hospitalizations or ER visits. Improvement on these metrics indicates that the care model is functioning as designed: managing conditions proactively before they generate acute events.
The California WPC pilot provides a useful framework here. Improved diabetes control, better blood pressure management, and higher rates of follow-up after mental health hospitalizations were among the documented outcomes, alongside the utilization reductions noted above.
Utilization and Cost
Lower ER utilization, reduced inpatient admissions, and decreased specialist dependency are the primary financial indicators of a well-functioning whole person care program. These metrics should be tracked against a comparable baseline population to distinguish program effects from broader trends.
For employers, reduced absenteeism and improved workforce productivity are meaningful secondary metrics. For health plans, the total cost of care per member per month is the primary financial benchmark, evaluated against Enhanced Care Management enrollment and engagement rates.
Engagement
A program that members do not use cannot produce outcomes. Galileo achieves over 40% engagement in populations where more than half of the members are being treated for chronic conditions. Engagement rates of this level, in high-complexity populations, reflect both the accessibility of the care model and the quality of the clinical relationships it builds.
Whole Person Care for Health Plans: CalAIM Alignment
For health plans operating in California, the connection between whole person care and CalAIM compliance is direct. DHCS requires managed care plans to provide Enhanced Care Management for targeted high-need beneficiaries, coordinate care across health, behavioral health, and social services, and engage community-based providers in delivering these services.
A whole person care partner with demonstrated infrastructure (unified records, multidisciplinary teams, multi-setting delivery, and real-time data sharing) provides the operational foundation health plans need to meet these requirements reliably and at scale. Health plans that attempt to fulfill ECM requirements through fragmented point solutions face the same coordination failures the program is designed to eliminate.
For health plans outside California, the CalAIM framework remains a useful reference point: it represents the direction of travel for Medicaid managed care policy nationally, with similar whole-person, value-based care requirements emerging in other states.
Building a Care Model That Actually Works
The evidence for whole person care is consistent across both public and commercial populations: coordinating physical health, behavioral health, and social needs produces better outcomes and lower costs than fragmented alternatives. California's WPC pilot demonstrated this for high-risk Medicaid populations. Galileo's outcomes data demonstrates it for employer and health plan populations across all 50 states.
What distinguishes programs that deliver results from those that do not is infrastructure: unified records, multidisciplinary teams, multi-setting care delivery, and the clinical intelligence to manage complex populations proactively rather than reactively.
To learn how Galileo's whole person care model can be structured for your workforce or member population, contact the Galileo partnerships team.



.webp)














%20(1).webp)
%20(1).webp)












.webp)