- Cost containment is the top strategic priority for health plan executives for the second consecutive year, driven by medical cost trends at 15-year highs, according to the HealthEdge 2026 Annual Payer Report.
- Three out of four health plan actuaries identify managing total cost of care as their primary cost deflation strategy, per PwC's Medical Cost Trend: Behind the Numbers 2026.
- Advanced primary care, contracted as a network strategy rather than a point solution, is one of the most structurally effective mechanisms for reducing the total cost of care across attributed member populations.
- A February 2026 report co-funded by the Milbank Memorial Fund and The Physicians Foundation found that adults with chronic disease who have consistent primary care access incur nearly 54% lower total healthcare costs and face a 20% lower hospitalization rate than those without it.
Healthcare cost containment is the systematic application of payment model design, network strategy, utilization management, and population health infrastructure to reduce unnecessary medical expenditure without compromising care quality or member access.
For health plans navigating medical cost trends at their highest sustained levels in more than a decade, advanced primary care solutions contracted at the network level represent one of the most structurally effective levers available for managing total cost of care across a defined member population.
The Cost Containment Imperative for Health Plans in 2026
Medical cost trend is hovering at rates reminiscent of 15 years ago, with commercial payers facing sustained pressure from medical services inflation and prescription drug costs that show no signs of moderating.
- For the second consecutive year, cost containment is the top priority for health plan executives across commercial, government, and dual-eligible plans, according to the HealthEdge 2026 Annual Payer Report.
- Healthcare represents nearly one in every five dollars spent in the U.S. economy, shared across the federal government (31%), state and local governments (16%), employers (18%), individuals (6%), and other payers.
- Three out of four health plan actuaries identify managing total cost of care as a primary cost deflation strategy, with payers deploying utilization management, claims integrity reviews, and pharmacy oversight programs in response.
The One Big Beautiful Bill Act (OBBBA) introduces more dynamic eligibility requirements and real-time enrollment validations, prompting health plan leaders to rethink how they manage data, collaborate with providers, and assess risk. Federal cost containment policy has not produced meaningful structural relief, and there is little expectation for significant legislative action in the near term.
Primary Cost Drivers for Commercial Health Plans
Six categories consistently drive the preponderance of claims spend across commercial plan populations:
Healthcare Cost Containment Strategies for Health Plans
Advanced Primary Care as a Network Strategy
Primary care represents less than 5% of total U.S. healthcare expenditures, yet it is the clinical setting with the greatest structural capacity to influence the 95% of spending that flows through specialist, hospital, and emergency care.
A February 2026 report co-funded by the Milbank Memorial Fund and The Physicians Foundation found that adults with chronic disease with consistent primary care access incur nearly 54% lower total healthcare costs and face a 20% lower likelihood of hospitalization. For health plans where chronic conditions drive the majority of cost trend, that differential is a direct actuarial argument for advanced primary care network investment.
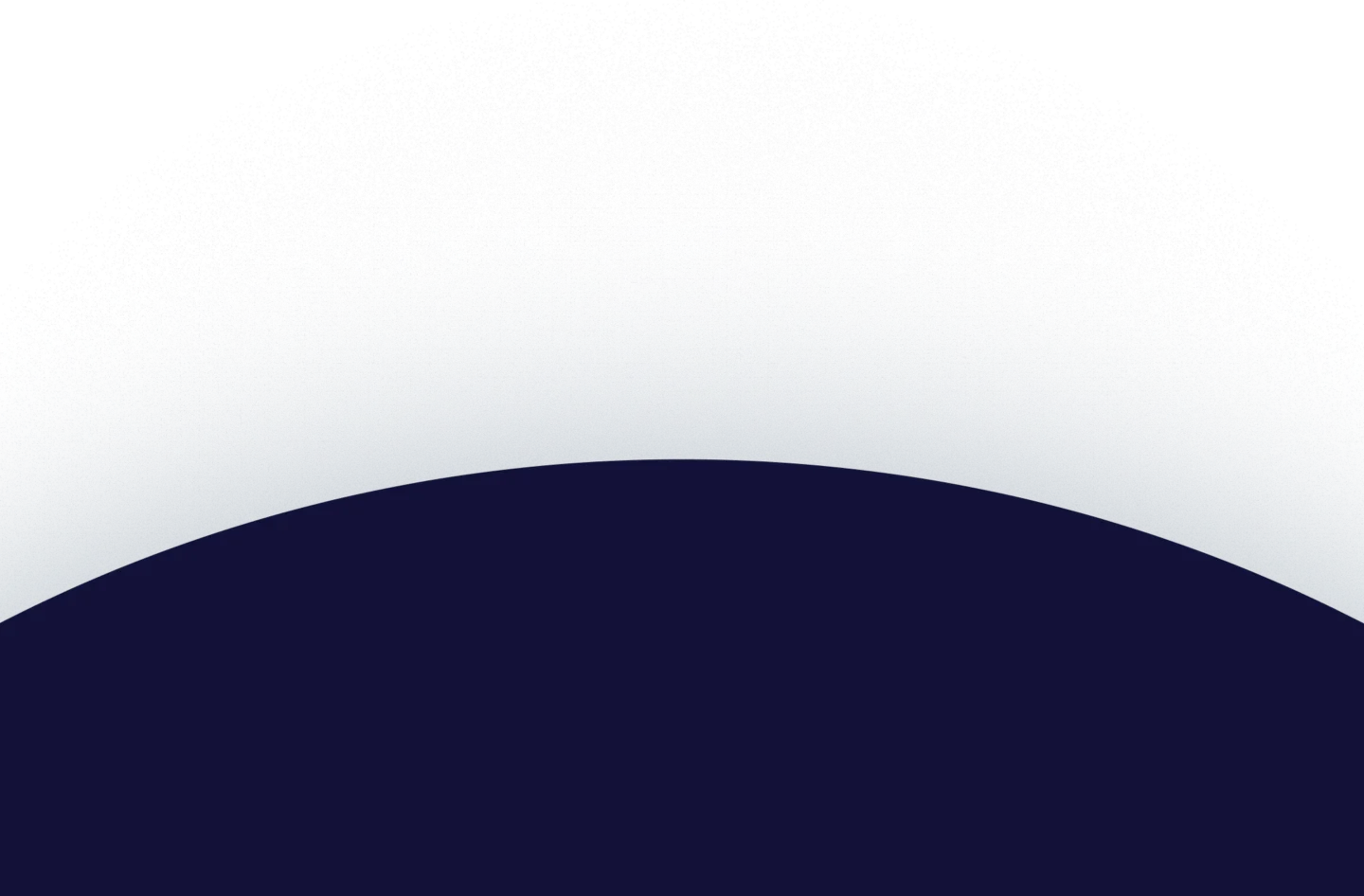
When contracted as a network strategy, advanced primary care delivers:
- 24/7 virtual access that resolves acute concerns before they generate emergency department or urgent care claims.
- Multidisciplinary team coverage spanning primary care, behavioral health, and chronic disease management within a single care environment, reducing specialist referral volume and duplicated testing.
- Proactive population outreach that identifies members with care gaps or poorly controlled conditions before they generate high-acuity events.
- Longitudinal care relationships attributed to a consistent care team with full clinical history, reducing fragmentation-driven overutilization.
Galileo's network data shows that 78% of patients choose Galileo over urgent care centers, ERs, or specialist providers, and 87% of cases are resolved without an in-person visit.
Value-Based Provider Contracting
Value-based contracts align provider financial incentives with the plan's cost containment objectives. The three primary structures available to health plans:
Shared savings (upside only): Providers earn a share of savings when they manage the attributed population's cost below a pre-established benchmark, with fee-for-service retained as the reimbursement base. This structure is typically the first step in health plan VBC contracting, as it allows providers to build population health capabilities without taking on downside financial risk.
Two-sided risk: Providers share in savings above the benchmark and bear financial accountability when costs exceed it. Creates stronger incentives for proactive care management investment, commonly used in ACO arrangements.
Capitation: A risk-adjusted, fixed payment per attributed member per period, regardless of services delivered. Offers the highest potential for incentive alignment and requires the most robust provider population health infrastructure.
Utilization Management
A broad prior authorization application alone creates an administrative burden, delays care, and generates member dissatisfaction without producing proportionate cost savings. Evidence-based utilization management targets high-cost, high-variation services where clinical criteria are well-established:
- High-cost imaging (MRI, CT), where watchful waiting or conservative care is clinically appropriate as a first step.
- Specialty pharmacy, particularly GLP-1 medications and oncology therapies, where step therapy requirements generate meaningful cost management.
- Elective surgical procedures in MSK categories where conservative care pathways have comparable outcomes at significantly lower cost.
- Specialist referrals for conditions manageable within advanced primary care.
The most effective UM programs pair prior authorization frameworks with care navigation support that helps members access the right care setting, rather than simply denying access to the wrong one.
Pharmacy Benefit Management
Specialty pharmacy spending is the fastest-growing component of medical cost trend for commercial health plans. Effective plan-level pharmacy cost containment requires:
- Transparent PBM contracting in which rebate economics are fully disclosed and rebates flow to the plan rather than the intermediary.
- Formulary management that prioritizes generics and biosimilars in therapeutic categories where interchangeable options exist.
- Specialty drug prior authorization with evidence-based clinical criteria and step therapy requirements.
- GLP-1 management programs with defined coverage criteria, outcomes monitoring, and integration with chronic condition management.
Population Health Infrastructure
Proactive cost containment depends on an integrated data architecture linking clinical, claims, pharmacy, and eligibility data to identify high-risk members before they generate high-cost claims. Core infrastructure components include:
- Risk stratification models using claims history, diagnostic codes, pharmacy data, and social determinants to prioritize outreach and care management enrollment.
- Care gap identification flagging members overdue for preventive screenings, medication refills, or chronic condition monitoring.
- Real-time eligibility integration ensures care management programs reach currently enrolled members.
- Quality measure tracking across HEDIS and other standardized frameworks to monitor clinical quality metrics that predict long-term cost outcomes.
Galileo achieves over 40% engagement in populations where more than half of members carry chronic conditions, using proprietary clinical software and integrated data flows to support accurate diagnosis and proactive care management at scale.
Build a Cost Containment Program Designed for Plan-Level Performance
Galileo operates as an advanced primary care solution for health plans and self-funded employers, with a multidisciplinary care team model, 24/7 virtual access across all 50 states, and integrated data capabilities built for population-level cost and quality reporting.
With over 40% engagement in high-acuity member populations and demonstrated reductions in emergency and urgent care utilization, Galileo is structured to serve as the primary care foundation of a durable plan-level cost containment strategy.
Connect with Galileo's health plan partnerships team to learn how an advanced primary care model can reduce the total cost of care across your attributed member population.



.webp)













%20(1).webp)
%20(1).webp)












.webp)