- Average per-employee healthcare costs reached $17,496 in 2025, a 6% increase, with a further 6.7% rise projected for 2026, per Mercer's 2025 National Survey of Employer-Sponsored Health Plans.
- Care fragmentation, avoidable ER utilization, and unmanaged chronic conditions are the three primary structural drivers of employer healthcare cost growth.
- Chronic and mental health conditions account for 90% of U.S. healthcare spending, making proactive chronic condition management the highest-leverage cost reduction intervention for most employer populations.
- Cost-shifting strategies, including higher deductibles and copays, suppress near-term utilization but generate higher downstream claims when employees defer necessary care.
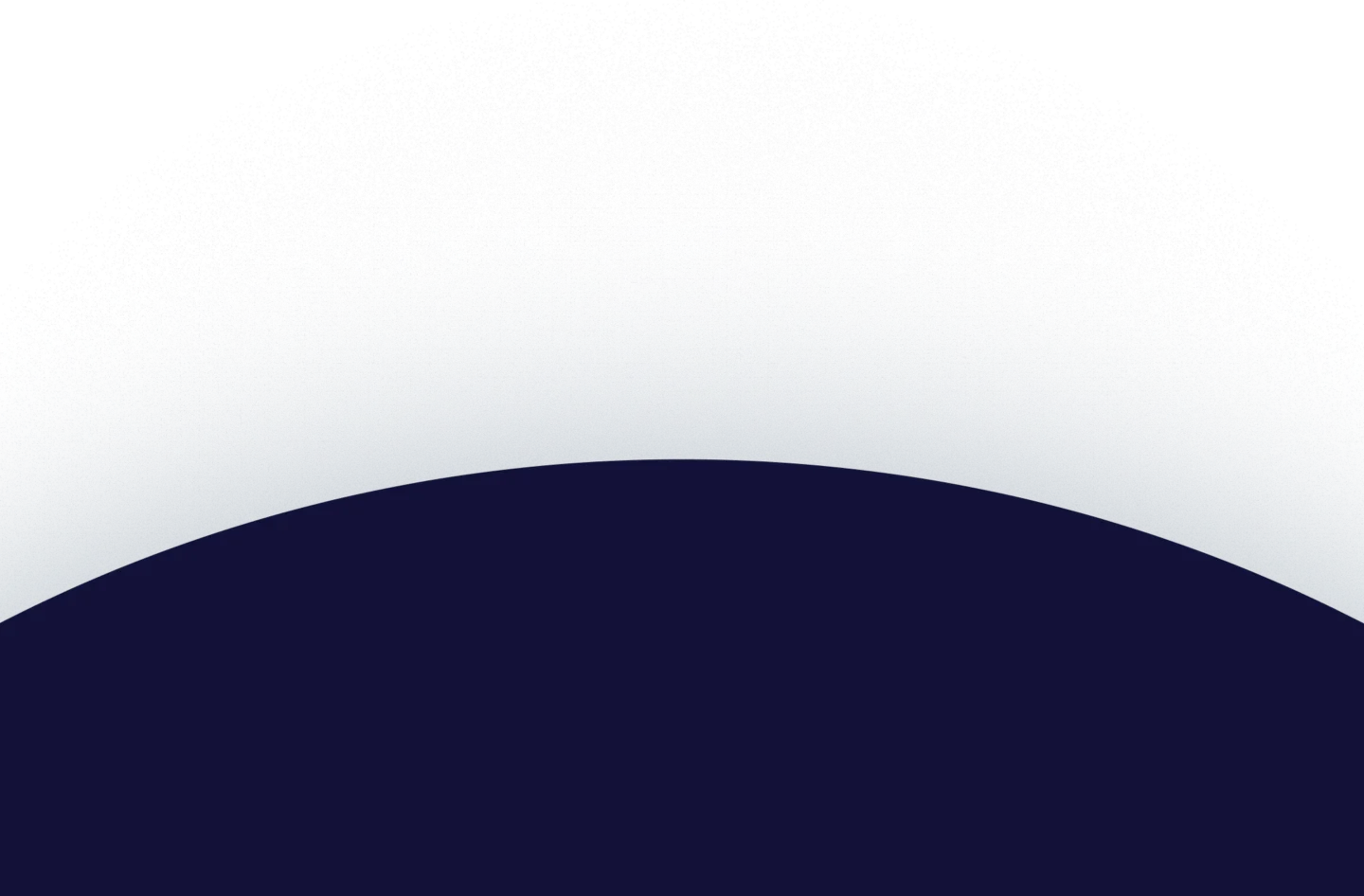
- Advanced primary care, with 24/7 access and proactive population management, is the most scalable structural solution for reducing avoidable utilization and total cost of care.
Employer healthcare costs are rising faster than wages, inflation, and most other operating expenses. Advanced primary care solutions that combine proactive population management with 24/7 access offer a structurally different approach: reducing unnecessary utilization at the point of care rather than shifting costs to employees or restricting benefits.
This guide examines what is driving employer healthcare costs, which reduction strategies carry the strongest evidence base, and how to implement a program that produces measurable, durable results.
Why Employer Healthcare Costs Keep Rising
The cost trajectory is not a temporary anomaly. Per Mercer's 2025 National Survey of Employer-Sponsored Health Plans, average per-employee healthcare costs reached $17,496 in 2025, a 6% increase over 2024, driven by prescription drug spending that rose 9.4% among large employers. A further 6.7% increase is projected for 2026, the highest in 15 years, pushing average costs above $18,500 per employee.
Three structural drivers account for the majority of that growth.
Fragmented Care
When employees navigate disconnected providers who do not share records or coordinate treatment, tests get duplicated, medications conflict, and conditions go unmanaged between specialist visits. Each coordination gap generates both clinical risk and financial waste.
Avoidable ER and Urgent Care Utilization
Many employees default to emergency departments for conditions that primary care can address more effectively and at a fraction of the cost. This pattern is driven by access barriers: when employees cannot reach a clinician quickly, they default to the most accessible high-cost setting.
Unmanaged Chronic Conditions
Chronic and mental health conditions account for 90% of U.S. healthcare spending, according to CDC data. Without proactive management, conditions like diabetes, hypertension, and behavioral health disorders worsen between appointments, generating hospitalizations, complications, and disability claims that represent the most expensive claims in employer health plans.
The fee-for-service payment model compounds all three. When providers are reimbursed per procedure rather than per outcome, there is no financial incentive to prevent unnecessary utilization, coordinate care proactively, or keep employees healthy between visits.
Why Cost-Shifting Does Not Solve the Problem
The most commonly deployed employer response to rising healthcare costs is increasing employee cost-sharing through higher deductibles and out-of-pocket maximums. The evidence consistently shows this approach backfires.
When employees face meaningful financial barriers to care, they defer treatment. Deferred treatment allows conditions to worsen. Worsened conditions generate the high-acuity acute events, hospitalizations, and emergency visits that are the actual drivers of employer healthcare claims spend. The near-term utilization suppression that higher cost-sharing produces is consistently offset by higher downstream claims costs.
The more productive question is not how much financial risk can be transferred to employees, but how benefit design and care delivery can reduce the volume and acuity of claims being generated in the first place.
Healthcare Cost Reduction Strategies That Work
Advanced Primary Care as the Cost Reduction Foundation
Primary care represents less than 5% of total U.S. healthcare expenditures, per a February 2026 report co-funded by the Milbank Memorial Fund and The Physicians Foundation, yet it is the clinical setting with the greatest structural capacity to influence the 95% of spending that flows through specialist, hospital, and emergency care.
The same report found that adults with chronic disease who have consistent primary care access incur nearly 54% lower total healthcare costs and face a 20% lower likelihood of hospitalization than those without it.
Advanced primary care extends this impact through:
- 24/7 virtual access that resolves acute concerns before they generate emergency department or urgent care claims.
- Multidisciplinary team coverage spanning primary care, behavioral health, and chronic disease management within a single care environment.
- Proactive population outreach identifies members with care gaps or poorly controlled conditions before they generate high-acuity events.
- Longitudinal care relationships with a consistent care team that knows each member's history, medications, and risk profile over time.
Galileo's data shows that 78% of patients choose Galileo over urgent care centers, ERs, or specialist providers, and 87% of cases are resolved without an in-person visit. For self-funded employers, that deflection translates directly to reduced claims.
Proactive Chronic Condition Management
Chronic conditions are the primary mechanism through which employer healthcare costs escalate. The path from an unmanaged chronic condition to a high-cost hospitalization is well-documented and highly preventable with consistent care management.
Effective chronic condition management requires care teams that do not wait for employees to schedule appointments. Proactive outreach, medication adherence monitoring, regular condition review, and timely specialist coordination when warranted reduce the frequency and severity of acute episodes before they generate high-cost claims.
Galileo achieves over 40% engagement in populations where more than half of members carry chronic conditions, using integrated data flows and proprietary clinical software to support consistent, accurate care management at scale.
Behavioral Health Integration
Behavioral health conditions, including depression, anxiety, and substance use disorders, drive significant employer costs through direct treatment expenses, disability claims, absenteeism, and lost productivity. Yet most employer health plans treat behavioral health as separate from physical health, creating access barriers and coordination gaps that amplify both clinical and financial costs.
Integrated behavioral health embeds mental health services within primary care so that employees can address both physical and behavioral health needs within a single care relationship, without separate referrals, separate networks, or weeks-long wait times.
This integration matters because mental and physical health conditions interact directly. Poorly managed depression worsens diabetes control. Unaddressed anxiety amplifies chronic pain. Treating the whole person reduces total claims across both categories.
Benefit Design That Incentivizes High-Value Care
Benefit design shapes the utilization patterns that generate claims. Employers with the most effective cost reduction programs design benefit structures that make high-value, appropriate-acuity care the financially preferred path for employees:
- Low or no cost-sharing for primary care visits, removing financial deterrents to early intervention.
- Tiered cost-sharing that creates financial incentives for using high-quality, cost-efficient providers.
- Centers of excellence programs for high-cost conditions (cancer, cardiac surgery, orthopedics) that direct complex cases to providers with demonstrated quality and cost efficiency.
- Formulary management prioritizing generics and biosimilars with appropriate prior authorization for high-cost specialty medications.
Self-Funded Plan Structure and Claims Data Visibility
Employers cannot reduce what they cannot measure. Self-funded or level-funded plan structures give employers direct visibility into their claims data, enabling targeted interventions rather than reactive premium adjustments.
The 2025 KFF Employer Health Benefits Survey reports that 67% of covered workers are now enrolled in self-funded plans. For employers still on fully insured arrangements, transitioning to self-funding is the foundational move that makes all subsequent data-driven cost reduction strategies possible.
Measuring What Matters
Effective healthcare cost reduction requires consistent measurement against defined benchmarks. The metrics that matter:
- Total cost of care per member per year: The primary financial outcome metric. Tracks all medical and pharmacy spend for the covered population.
- ER and urgent care utilization rates: Avoidable emergency department visits per 1,000 members, tracked against national benchmarks over time.
- Preventive care completion rates: Leading indicator of chronic condition control and long-term cost trajectory.
- Chronic condition control metrics: HbA1c levels, blood pressure control, and medication adherence rates for members with high-cost conditions.
- Member engagement rates: Visit frequency and activation rates indicate whether employees are actually using the program.
- Generic dispensing rate: Proportion of prescriptions filled with generics, a direct indicator of pharmacy cost management effectiveness.
Implementation: From Strategy to Measurable Results
Reducing employer healthcare costs requires a sequenced strategy, not a single procurement decision.
- Step 1: Establish claims data visibility: Transition to a self-funded or level-funded structure that provides direct access to medical and pharmacy claims. This is the prerequisite for every subsequent data-driven intervention.
- Step 2: Stratify the population by cost and risk: Use claims data to identify the conditions, utilization patterns, and member cohorts driving the majority of spend.
- Step 3: Deploy primary care infrastructure capable of proactive management: Select a care delivery partner with 24/7 access, multidisciplinary team coverage, and the data capabilities to engage high-risk members before they generate high-acuity claims.
- Step 4: Redesign benefit incentives to reward high-value care: Make primary care and preventive engagement the financially preferred path for plan members.
- Step 5: Align provider payment with outcomes: Move toward value-based care arrangements beginning with shared savings models, progressing toward greater accountability as performance data accumulates.
- Step 6: Measure quarterly against defined benchmarks: Review total cost of care, utilization patterns, quality metrics, and engagement rates on a defined reporting cycle.
Reduce Healthcare Costs at the Source, Not on the Statement
Employer healthcare costs will not moderate through plan design adjustments alone. The conditions, utilization patterns, and care fragmentation driving claims require a care delivery model structurally built to address them before they reach the claims statement.
Galileo operates as an advanced primary care solution for self-funded employers and health plans, with a multidisciplinary care team model, 24/7 virtual access across all 50 states, and integrated data capabilities built for population-level cost and quality reporting.
Connect with Galileo's employer partnerships team to learn how an advanced primary care model can reduce the total cost of care for your population.



.webp)













%20(1).webp)
%20(1).webp)












.webp)